
Plagiocephaly Information for Providers
Boston Orthotics & Prosthetics has extensive experience in the management of deformational plagiocephaly through our clinical network, and is bringing progressive designs and techniques forward to advance the treatment options for this pediatric population.
Boston O&P is the only company that offers several options for both the prevention and treatment of plagiocephaly, including products designed to avoid plagiocephaly and an affordable helmet solution that achieves results quickly and effectively when plagiocephaly has already occurred.
Types of Cranial Asymmetry
Head shape is commonly described using terms of Latin origin. The four shapes described below are the most common abnormal head shapes a pediatrician will see. These four abnormal head shapes can be caused by either mechanical cranial deformation or by craniosynostosis, a condition caused by premature closure of a cranial suture (growth plate). Craniosynostosis is rare, and needs to be diagnosed and followed by a specialist.
Plagiocephaly
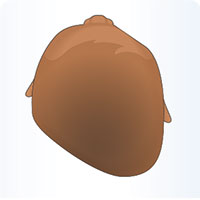 The term plagiocephaly describes an “oblique”head. This can be predominantly anterior (forehead flattening) or posterior (parietal flattening). Posterior deformational plagiocephaly is the most common abnormal head shape a pediatrician will see. Flattening is accompanied by anterior displacement of the ear on the same side as the flattening forehead, and in severe cases, the orbit and cheek. When the ear on the opposite side of the flattening is further forward, a specialist should be sought to rule out synostosis.
The term plagiocephaly describes an “oblique”head. This can be predominantly anterior (forehead flattening) or posterior (parietal flattening). Posterior deformational plagiocephaly is the most common abnormal head shape a pediatrician will see. Flattening is accompanied by anterior displacement of the ear on the same side as the flattening forehead, and in severe cases, the orbit and cheek. When the ear on the opposite side of the flattening is further forward, a specialist should be sought to rule out synostosis.
Brachycephaly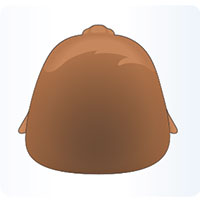
Brachycephaly describes a short, wide head. The occiput flattens and there is bilateral widening in the temporo-parietal regions. In deformational brachycephaly, there is often bulging above the ears.
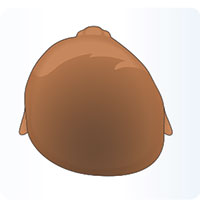 Asymmetric Brachycephaly
Asymmetric Brachycephaly
Asymmetric brachycephaly is the combination of plagiocephaly and brachycephaly. It is characterized by asymmetric occipital flattening accompanied by parietal flattening on the same side.
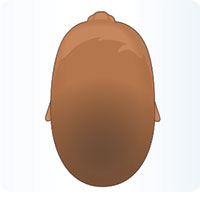 Scaphocephaly
Scaphocephaly
Scaphocephaly (also known as “dolichocephaly”) is characterized by flattening of the sides of the head and elongation from anterior to posterior. Deformational scaphocephaly is most often seen in premature infants.
Causes of Plagiocephaly
Understanding risk factors for deformational plagiocephaly is essential for prevention, diagnosis, and treatment. While there are many ways infants can develop cranial asymmetries, the common denominator is that growth is restricted in a fixed area of the head. While supine sleeping is often blamed for causing cranial deformation, multiple risk factors are usually present in infants with plagiocephaly.
Some Causes of Cranial Asymmetry
- Position in the womb
- Developmental delays
- Poor muscle tone
- Spine abnormalities
- Back sleeping
- Torticollis: a tightness of the sterno-cleido-mastoid muscle on one side of the head that causes the child to look toward the contralateral shoulder, causing the contralateral side to become deformed. Because torticollis (sternocleidomastoid muscle imbalance) is a strong risk factor for deformational plagiocephaly, primary providers should ask whether or not the infant has a head positional preference during the first well-baby visit.
A preferred head position, or difference in cervical rotation may be a sign of torticollis. Even in the absence of limited cervical rotation, positional preference is often associated with deformational plagiocephaly.
Risk Factors for Developing Plagiocephaly
- Multiple births
- Firstborn children
- Breech births
- Premature births
- Male infants
- Long labors
- Infants who spend time in a neo-natal intensive care unit (NICU)
- Restricted movement while supine (such as in a car seat, swing, or crib)
Prevention/Treatment Options
In cases that are identified very early on or when the child is predisposed to have positional cranial flattening (premature birth, multiple birth, in NICU for a period of time at/after birth), Boston Orthotics & Prosthetics advocates repositioning techniques including:
- The Crown Cradle: is intended exclusively for use for babies in hospital neo-natal Intensive Care Units.
- The Perfect Noggin: the most ergonomic and clinically effective sleep surface available to maintain a natural head shape in infants.
 If repositioning is unsuccessful, Boston O&P offers excellent an effective treatment option:
If repositioning is unsuccessful, Boston O&P offers excellent an effective treatment option:
- The Boston Band: a lightweight, plastic and foam orthosis made from a cast impression or a 3D scan of the infant’s head.
Concerns for Pediatricians
Many of our patient referrals come from specialists such as cranio-facial surgeons, but a growing number of our patient referrals come directly from pediatricians. This is a widely accepted practice because in the vast majority of cases, the deformation is truly positional and there are no other underlying concerns.
Why then have some pediatricians been reluctant to use this treatment? Well, some forms of synostosis (premature closure of the cranial sutures) can appearance to be plagiocephaly, such as:
Unilateral coronal syntosis:
In this example. the left coronal suture is prematurely fused and therefore no more growth can occur from this suture line. This shows a slightly posterior plagiocephaly on the left side however in true positional plagiocephaly you would also see a left anterior bossing (pushing forward all on the same side). In this case, the anterior bossing in only on the child's right side. This is fairly obvious and indicates something other than positional deformity. Reports vary, but this is thought to be seen in only one in 3,500 live births.
Unilateral lambdoidal synostosis
In this example, the right lambdoidal suture prematurely fuses. You see the posterior flattening that would seem to indicate right plagiocephaly, however upon further review you notice a couple things conflicting with that diagnosis:
- The anterior bossing is on the forehead while the right is actually sunken back.
- The right ear may actually be shifted posteriorly also. Remember, in true positional plagiocephaly, that forward shift is all on the same side. The means the right ear and right forehead would be shifted forward if it was positional plagiocephaly. Again, reports vary, but this configuration is thought to occur in only one in 100,000 live births.
Sagittal synostosis and metopic synostosis
Sagittal synostosis (shown) and metopic synostosis are also potential forms of synostosis, however obviously do not in any way mimic deformational plagiocephaly. They are the most common forms of prematurely closed cranial sutures, occurring in one in 2,000 live births and one in 2,500-3,500 live births respectively.
Please understand that we are in no way discouraging use of specialists, however we are saying that in many cases, a pediatrician with proper training can make the diagnosis of positional cranial deformity versus synostosis and refer the patient directly to an orthotist if a cranial remolding orthosis is warranted. This process obviously saves time and money. If there is any doubt whatsoever or co-morbidities present, please contact a specialist immediately.
Publications & Articles
- Comparison of Helmet Therapy and Counter Positioning for Deformational Plagiocephaly, Annals of Rehabilitation Medicine, 2013
- Congress of Neurological Surgeons Systematic Review and Evidence-Based Guideline for the Management of Patients With Positional Plagiocephaly: The Role of Physical Therapy, Congress of Neurological Surgeons, 2016
- Congress of Neurological Surgeons Systematic Review and Evidence-Based Guideline on the Role of Cranial Molding Orthosis (Helmet) Therapy for Patients With Positional Plagiocephaly, Congress of Neurological Surgeons, 2016
- Congress of Neurological Surgeons Systematic Review and Evidence-Based Guideline on the Management of Patients With Positional Plagiocephaly: The Role of Repositioning, Congress of Neurological Surgeons, 2016
- Effectiveness of Conservative Therapy and Helmet Therapy for Positional Cranial Deformation, PRS Journal, 2014