
Dynamic Movement Orthosis (DMO) Information for Providers
Dynamic Movement Orthoses (DMO) is a new way to look at bracing. Traditional braces typically either hold a certain body segment in place or prevent an undesired movement or posture. DMOs allow guided movement allowing the patient, and more important their motor pathways, to work themselves to make the desired motion occur. The trick is it encourages the wearer to do the things we would like to see them do. For example, some children have trouble opening their hand, grasping a toy and then releasing that toy to pick up another one. The DMO can be designed to help do just that. The difference is it helps the wearer to do these things better and more often.
Over time, the goal is they will be able to do these things without assistance from any external device because they have trained themselves how to do it correctly. Wearers do not always gain this ability, however it has been attained by many. Independence! Regardless, greater functional ability and/or posture are the goals.
What are DMOs made of?
Very basic materials, mostly lycra. It is soft, comfortable, and light. Thicker than control top panty hose however thinner than Isotoner gloves. DMOs do not interfere with anything and can fit underneath any piece of clothing or shoe.
What styles are available?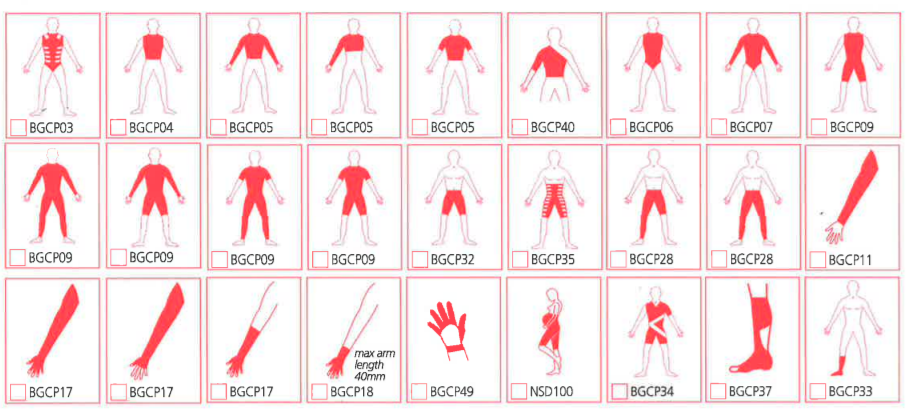
Basically anything. The DMO can be a simple “glove” (traditionally called a wrist-hand orthosis), “sock” (ankle-foot orthosis), “suit” which is typically from the shoulders to the hips, or anything in between. The orthosis can include, or not include, whatever is necessary for that person.
The following DMOs are available through Boston O&P:
DMO Essentials
DMO Suits
DMO Sensory
How do DMOs work?
A DMO works in a variety of ways:
- The base layer of lycra provides compression to the entire body segment. This helps send more and better sensory information to the brain. For example, touch is a form of sensory information. When we touch something hot, our brain immediately tells us to stop touching it. The DMO helps send different sensory information, called proprioceptive sensory information to the brain. “Proprioception” means the person’s ability to know where their body is in space. This means the wearer will be more aware of where that body segment is (bodily awareness) and now will be able to relax. This helps reduce spasticity and high tone. Ironically, it can also help increase a persons level of tone if they tend to have low tone or are “floppy.” It does this the same way, through better proprioception. The wearer now understands they need to increase their muscle tone to achieve the goal (function, posture, or both).
- Over the base layer are other “panels.” These panels are put on based on the needs of the wearer. For example, if a person catches their toes with each step then we can add a panel which will help them lift their toes. Or, if the person tends to fall to a certain side while sitting, we can add panels to their “suit” to help them sit up and be steadier. The orthotist, therapist and physician should collaborate to design the best DMO for each individual.
How can this “soft” device overcome a child’s severe high tone when something with “stays” (rigid) doesn’t even work?
With high tone, stays can actually make matters worse. For example, sometimes when high tone meets resistance (the stays), the tone actually increases. They become uncomfortable and can cause redness in certain areas like on the wrist, or on the chest, etc. depending on the device. The DMO will help your child learn how to self-calm at the brain level and also help them relax in that particular body part. The DMO allows that undesirable posture temporarily which helps the wearer relax quicker. Upon relaxing, the DMO will help them achieve our desired goal (function, posture or both).
How can this “soft” device help a child sit up better or have a more stable hand/wrist or foot/ankle? Won't a larger child overpower the lycra?
Actually, your child’s size and weight don’t make much difference. The DMO is not designed to do “all the work.” The idea is that it helps “teach” your child to do it for themselves. Through the two means described in question #3, it helps put your child in position for success. Even small successes like holding a better position for a few seconds or doing a new task once. These small successes snowball into doing that one thing more or for longer periods of time. Remember, this is truly a re-training tool. Not something to manage the progression of the dysfunction.
Who can use DMOs?
We are only beginning to understand DMOs true reach however we have found it to be successful in quadriplegia, diplegia & hemiplegia with the following general presentations:
- High tone and/or spasticity
- Low tone
- Athetoid
- Ataxic
- Dystonic
- Mixed presentations
It is certainly not for everyone however a good rule of thumb is if you can help the person achieve that desired task using your hands then the DMO will be able to do the same thing, and probably better, because of the sensory feedback. Another rule of thumb is that if you, the potential wearer and your rehab professionals think you could be doing better than your current state or if your current orthotic intervention is causing other issues (like redness, skin breakdown, etc), a DMO may be a good thing to consider. Some people simply do not tolerate rigid braces. DMOs are like another piece of clothing that they will feel comfortable wearing.
We are happy to consult and give honest feedback based on our experiences. We can also share before and after video of patients that may have similar types of dysfunction and may have similar goals as your patients.
When can’t DMO be used?
DMOs have been used successfully in treating neuropathic scoliosis however they are not recommended for idiopathic scoliosis and should not to be used on rigid curves with large degrees of rotation. This should always be assessed by an orthotist that has experience and has been trained in the use of DMOs with neuromuscular scoliosis.
In bracing limbs, DMOs will not likely reduce any true range of motion deficit (contracture). It can absolutely help the wearer use all of their passive range of motion actively. It is designed to do this. The other known limitation is in the ankle. If the goal is to provide clearance of the toes when walking, the person needs to exhibit some ability to lift their toes on their own. If this is not possible then it is likely the device will not help that person with toe clearance and a more rigid device will be better.
How do we get a DMO?
The best way is to inquire to your physician, therapist, or orthotist. If all in agreement, your physician would need to write a prescription stating the type of device and the goal(s). Now we can design the DMO appropriately. If they are unaware of DMOs, please feel free to have them contact Customer Service at 800.262.2235. They can answer questions and even direct them to relevant patient video that may help in the decision making process.
Where can I get a DMO?
From any of our Certified Partners! Measuring for and providing DMOs is quite a challenge. We have trained a small group of orthotists based on their passion, ability, and geography. We wanted to make sure that any person that could benefit from a DMO could get it relatively local to them. We consider this group of orthotists our extended network. They have been instrumental in advancing our mission of improving patient care by providing insightful feedback, opening up their doors to us for discussion and hands-on training, and in documentation or results. This network is the only known network heavily focused on training and documenting evidence in order to improve patient care every day.